Biomechanics and Human Sexuality
Sir Isaac Newton’s laws of physics are critical to human sexuality. For example, Newton’s third law states, “If two bodies exert forces on each other, these forces have the same magnitude but opposite directions.” This allows for two people to physically stimulate each other during sex. Biomechanics is the application of a branch of physics known as “mechanics,” which includes Netwon’s laws, to biological systems. Thus, sex has a biomechanical component in addition to the psychological and relationship aspects.
However, biomechanics is more than just Newton’s laws applied to human-to-human contact. It also describes the motion of the entire body, explaining how and why it moves. It further explains how the tissues that make up sex organs deform in response to force. Very importantly, it explains how these tissue deformations are converted into nerve impulses that create the sensations associated with sex. Biomechanics also encompasses the mechanics of fluids and the rigidity of mechanical structures, both of which are central to achieving and maintaining an erection. Tribology, the study of friction, wear, and lubrication, can help explain all kinds of sex, from masturbation to partnered sex.
The relationship between sex, aging, and biomechanics may be less obvious. Adding age into the mix complicates this a bit, because it requires thinking about both the biomechanics of aging and the biomechanics of sex. There are two ways that increasing age affects the physical ability to have sex: (1) the natural biological processes of aging and (2) the life events that people experience as they age. For example, in men, the former may involve a reduced ability to achieve and maintain an erection, and the latter may involve side effects of surgical intervention for prostate cancer. For women, the former may involve reduced vaginal lubrication due to menopause, and the latter may involve the effects of vaginal childbirth on the pelvic floor muscles. I don’t make a distinction between the former and latter: that is for academics to do.
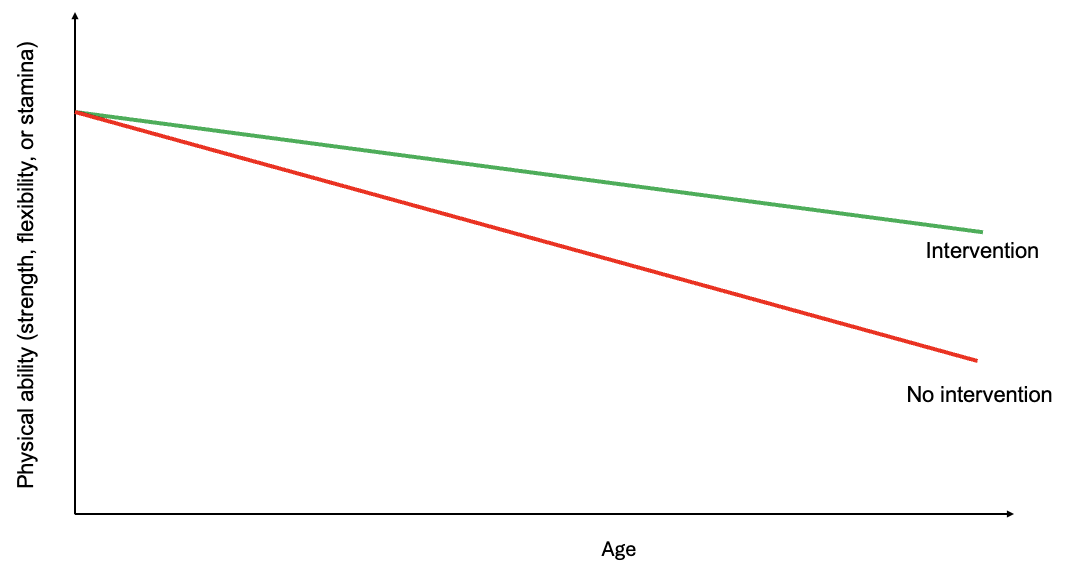
Figure 1. Conceptual model of how physical capabilities change with age through adulthood.
What is well documented is that changes in human biomechanics occur as we age, and these changes can affect our sexuality. However, we have control over many – if not most – of how these changes will affect our sex lives. It is not as if we are doomed to stop having sex at 50, 60, 70, or above because of how our bodies change. The example I like to use in lectures is hip strength and flexibility. Figure 1 shows, in cartoon form, what happens to hip flexibility and strength as we age: the red line shows that they decline without any “intervention.” Betty Dodson writes in her forward to Joan Price’s book, Naked at Our Age: Talking Out Loud About Senior Sex: “As I approached sixty, I felt a need to challenge the aging process more assertively. My hip joints were getting stiff and painful, and I was faced with a physical challenge.” I like Betty Dodson’s phrase “challenge the aging process more assertively” to describe an intervention. For the hip, the intervention can mean doing home- or gym-based exercises that target the hip. The green line indicates how hip function changes over time with the exercise intervention.
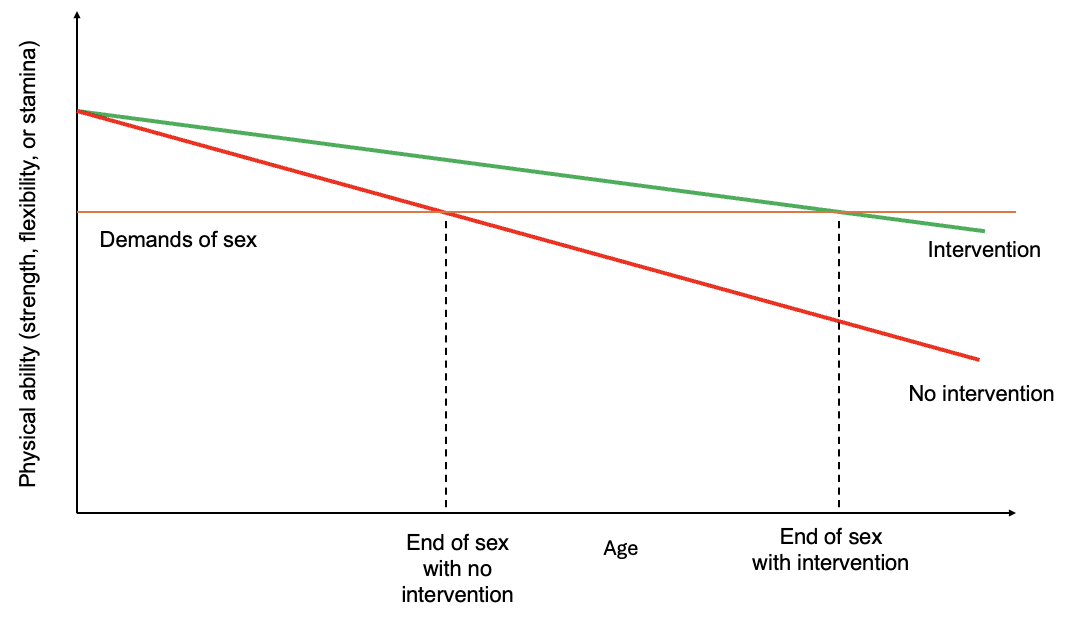
Figure 2. Conceptual model of when PIV sex ends with and without intervention.
Consider the example of penis-in-vagina (PIV) sex. PIV sex requires some level of hip function for both partners. Figure two shows a conceptual diagram of when sex would end for one of the partners. The orange line represents the hip’s physical requirement during PIV sex in a specific position. When physical capability falls below the physical demands, PIV sex isn’t possible in that position (“end of sex with no intervention”). Betty Dodson’s “challenging our aging” intervention extends the number of years that PIV sex is possible. This is biomechanics in action: exercise is an intervention to reduce the rate at which we lose hip physical capacity. Moreover, for many people who haven’t been very physically active, starting an exercise program can not only slow the loss of capacity but actually increase it.
One clear result of thinking about sex using biomechanics is that maintaining hip flexibility and strength is important. This applies to other joints as well, especially the lower (“lumbar”) spine, because controlling pelvic motion during PIV sex depends critically on what the hip and spine can do. This will be discussed in greater detail in a future post. An additional consequence of these two figures is that reducing the “demands of sex” can extend the age at which a person can’t engage in sex. Changing task demands falls within the field of “ergonomics,” and it will be discussed in the next blog post.
In addition to joint strength and flexibility, other biomechanical factors associated with sex affect our ability to have sex as we age. Some these include:
Post-operative precautions for some surgeries. Hip arthritis is very common in older populations and hip replacements are used to treat it. Due to the design of the artificial hip prosthesis, there are sexual positions that should be avoided to prevent dislocation of the prosthesis following surgery. The mechanism of dislocation is purely biomechanical, and biomechanical principles can be used to guide ergonomic interventions (i.e. changed sex positions) for the prevention of dislocation. The previous post on 2/5/26 addressed this topic.
Pelvic floor muscle strength. The pelvic floor muscles are often disrupted during vaginal childbirth. Research has shown an association between pelvic floor muscle strength and sexual function in women. Kegel exercises strengthen these muscles.
Menopause. Menopause has biomechanical consequences that affect sex. Most notably, it affects vaginal lubrication and vaginal wall mechanical properties. Reduced natural lubrication can make PIV sex painful. These changes are due to hormonal shifts, especially estrogen levels. I am not an endocrinologist, so I won’t give opinions on hormonal treatments. I will just suggest talking to your medical provider if this is of concern to you. Artificial lubricant - “sex lube” or “personal lubricant” – is also a way to address this.
Sensation. Skin has “mechanosensory” nerve endings that detect mechanical forces such as pressure and vibration. Their sensitivity declines with age, which can affect sexual response. For example, as the ability to sense mechanical stimulation decreases with age, additional stimulation may be required.
Penis function. Biomechanically, the penis involves biofluids and structural mechanics. Insights from biomechanical studies of the penis can inform treatments for erectile dysfunction. Mechanosensory aspects also influence the likelihood of using a condom during sex, thereby affecting sexually transmitted infection risk.
Orgasm. Muscle contraction is an important part of orgasm, both for men and women.
Balance. Many couples enjoy having sex in standing positions, which requires balance from at least one partner. The ability to maintain balance declines with age. Biomechanics can be applied to understand what forces should be applied to the surroundings (partner, floors, walls, railings, etc.) to maintain balance and safely have sex.
The mission of Sex and Aging Biomechanics is to educate people on how to use the principles of biomechanics and ergonomics to maintain active and healthy sex lives as they age. This post has been an introduction and overview of how biomechanics applies to sex and aging. It used PIV sex as an example, but the same principles apply to gay and lesbian sex. The next one will be about ergonomics and sex, and it will be based on the concepts introduced here. Each of the topics presented here will also be explored in detail in future blog posts. Most posts will be written for a non-technical audience. However, at times I won’t be able to resist also providing a technical, mathematical treatment of a topic. In that case, I will make a separate post with “(for nerds)” appended to the post title.