Sex After Hip Replacement

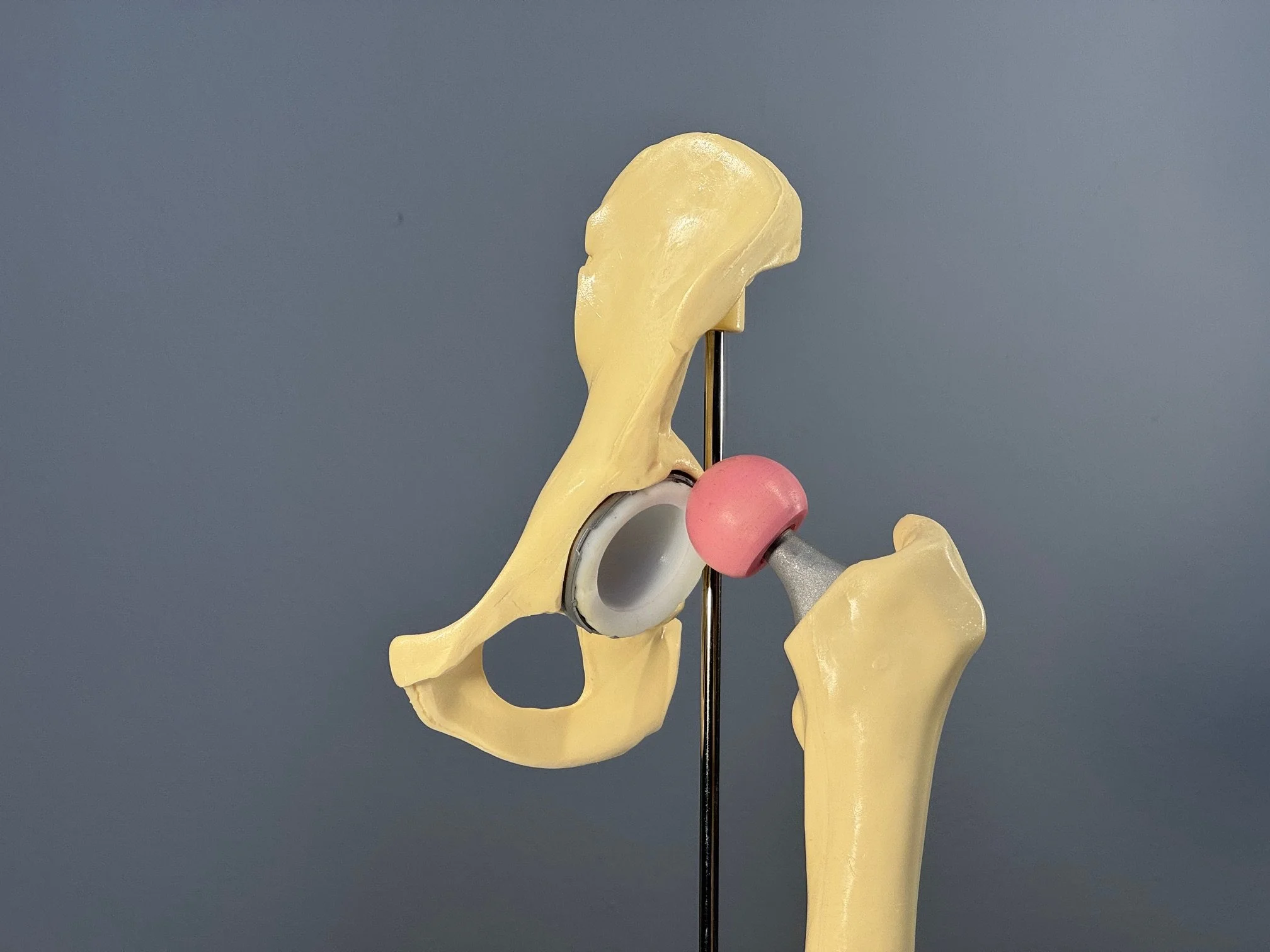
Plastic model of a total hip replacement. A cup is placed in the pelvis (a thin piece of metal seated inside the bone), and it is lined with plastic to reduce friction as the hip moves. The pink ball inside the plastic is the “head,” which sits on top of a metal stem that is inserted into the thigh bone.
Sex is possible after a total hip replacement, but some positions can put the newly implanted artificial hip at risk of coming apart. The good news is that this risk can be avoided by thoughtfully choosing sex positions. Orthopaedic surgeons refer to the implant “coming apart” as dislocation. It is not life-threatening, but it is painful and often requires a trip to the emergency room of a hospital to be resolved. If it happens multiple times, surgery might be required. It is something that patients don’t want to experience. The mechanism is biomechanical, which is why it is included in this blog. Orthopaedic surgeons often provide handouts to patients about sex positions that are low risk for dislocation to hip replacement patients. An excellent handout for this was developed by the American Association of Hip and Knee Surgeons (AAHKS). In addition to explaining the issue, it contains (non-explicit) diagrams of twelve sex positions and lists whether each poses a risk of prosthesis dislocation for the man and the woman. The American Academy of Orthopaedic Surgeons (AAOS), the main professional association of orthopaedic surgeons in the United States, also has a webpage with information. Hospitals and individual surgeon practices may develop their own handout or pamphlet.
Online educational resources are also available. A company, Ergoerotics, has a wonderful video titled “Sexual Ergonomics: Practical Strategies and Positions for Comfortable Pleasure. Volume 1: Hip and Knee Pain & Surgery” that shows sex positions that are low risk for dislocation. Moreover, a fully clothed couple demonstrates the positions and how to get into and out of them without putting the prosthesis in a vulnerable position. The videos were produced by an expert in human sexuality, Heather Howard, Ph.D., and clinical input was provided by an orthopaedic surgeon, Gordon Lundy, M.D. Although this video is behind a paywall, it is well worth watching if you and/or your partner have – or will have - a hip replacement.
Hip prosthesis dislocation is a biomechanical phenomenon. In some leg positions, the neck of the implant stem on the leg side touches the rim of the metal cup in the pelvis. The rim acts as a fulcrum of a lever system, and the forces acting on the leg “lever” the head of the implant out of the cup. Surgeons call the contact between the neck and cup “impingement.”
The forces involved in walking and moving force the head up beside the top of the cup.
The AAHKS-recommended sex positions have limitations, however. The most obvious limitation is that the study examined only penis-in-vagina (PIV) sex. The AAHKS handout is based on a study of a man and a woman engaging in “simulated” PIV sex in a motion capture laboratory. That study used volunteers who do not match the typical hip replacement patient in America. The man was 26 years old and weighed 176 pounds; the woman was 31 years old and weighed 152 lbs. Both study participants were the same height, 5’ 11”. For comparison, the average age of a hip replacement patient in Michigan is 66, and the average weight is 195 lbs. While this mismatch in age and weight does not invalidate the study and recommendations, it is something to consider when evaluating their applicability to a specific set of sex partners. An additional limitation is that these recommendations are heteronormative; they do not address gay and lesbian sex.
There is also a wonderful online resource addressing this topic. Heather Howard, Ph.D., created www.ergoerotics.com, which features a video titled “Hip and Knee Pain & Surgery.” It focuses on precautions to take following hip replacement surgery. In it, a couple demonstrates various PIV sex positions that reduce the risk of hip prosthesis dislocation. The couple is clothed, so it is not pornographic. Dr. Howard also provides commentary. What makes this resource superior to the AAHKS handout is that it specifically addresses how to get in and out of the sex positions without placing the hip in a problematic position. The downside to this video is that it is behind a paywall. As of today, the cost is $25.00 (USD) for three months of access.
Despite these resources, you may still have questions you would like to ask your orthopaedic surgeon about sex following hip replacement surgery. A study by orthopaedic surgeon Diane Dahm, M.D., and co-workers at the Mayo Clinic reported that 80% of hip replacement surgeons “rarely or never” talk to their patients about sex. If your surgeon doesn’t address sex following surgery, you can bring up the subject. In her book, “The Ultimate Guide to Sex after 50: How to Maintain – or Regain – a Spicy, Satisfying Sex Life,” Joan Price gives advice on how to talk to doctors about sex: “A doctor who is considerably younger may not view us as sexual beings and is likely to assume that we don’t’ have a sex life, or care about it. The doctor won’t think to ask us about sex, concentrating on helping us treat our ailments. It’s up to us to start the conversation. We can overcome our own reluctance by preparing ahead what we want to say. Writing down our questions is a good strategy. Then we need to assert ourselves. When another issue is the reason for the appointment, a good plan is to say at the beginning, ‘I have something else I want to discuss with you. Let’s leave time for that.’ Now you can’t back out. We must commit to bringing up our sexual issues assertively and unapologetically. Only this way we can help ourselves, help out doctors know what we need (and want!), and – ultimately – help our generation and those that follow.” She also quotes some sage advice from sex therapist Marty Klein, Ph.D., “Let the docs deal with their discomfort. They’re getting paid.” It can also be useful to ask the clinic’s staff, such as physician assistants and nurses, if asking the surgeon is too uncomfortable. This may be the case if your surgeon is a different gender than you. It is OK to ask to ask clinic staff if that feels better to you.